Method validation of an inductively coupled plasma mass spectrometry (ICP-MS) assay for the analysis of magnesium, copper and zinc in red blood cells

Journal of Mass Spectrometry and Advances in the Clinical Lab, Volume 34, 2024: Fig. 1. Accuracy study – Linear regression and Bias plots, magnesium (A), Copper (B) and Zinc (C).
The goal of this study is to develop and validate a reliable analytical method using inductively coupled plasma mass spectrometry (ICP-MS) to quantify magnesium (Mg), copper (Cu), and zinc (Zn) in red blood cells (RBCs). Accurate measurement of these trace elements is essential for evaluating nutritional status and detecting potential metal toxicity.
Through method validation—including assessments of accuracy, precision, linearity, and sensitivity—the study confirms that the assay meets clinical standards. Retrospective analysis of patient data further supports the method’s clinical utility, revealing significant differences in trace element levels across age and sex groups. The validated method offers a robust tool for clinical evaluation of trace element status.
The original article
Method validation of an inductively coupled plasma mass spectrometry (ICP-MS) assay for the analysis of magnesium, copper and zinc in red blood cells
Nazmin Bithi, Daniel Ricks, Brandon S. Walker, Christian Law, Kamisha L. Johnson-Davis
Journal of Mass Spectrometry and Advances in the Clinical Lab, Volume 34, 2024
https://doi.org/10.1016/j.jmsacl.2024.10.003
licensed under CC-BY 4.0
Selected sections from the article follow. Formats and hyperlinks were adapted from the original.
Trace elements play a critical role in human growth and development, even in small quantities. These elements primarily act as catalysts in various enzymatic reactions within the body. It is essential to ensure an adequate supply of these essential trace elements to maintain a high quality of life [1]. Thus, clinical measurement of trace elements is helpful in nutritional assessment and may be necessary for determining potential deficiencies and/or toxicities for patient management. Laboratory assessments of microelements, such as magnesium (Mg) and trace elements like copper (Cu) and zinc (Zn) in red blood cells (RBCs) are utilized to evaluate patients' nutritional statuses [2]. Hemodialysis patients commonly face systemic Zn deficiency. However, solely monitoring plasma Zn levels may fail to consider intricate interactions occurring within RBCs. Improper Zn supplementation may potentially result in Cu deficiency, underscoring the importance of maintaining balanced levels. To gain comprehensive nutritional insights, it is crucial to recognize systemic Zn deficiency and evaluate Zn and Cu dynamics within RBCs [3]. Therefore, measuring multiple elements in RBCs, such as Mg, Cu, and Zn, collectively provides insights into the intracellular stores and overall homeostasis levels of these essential minerals.
Mg is the fourth most abundant cation in the human body and is considered an essential mineral [4], serving as a cofactor for over 325 enzymatic reactions in cells [5]. It is found in various foods, including fruits, vegetables, nuts, meats, fish, and dairy products, as well as in drinking water. Mg plays a vital physiological role in calcium and potassium transport, cell signaling, and energy metabolism in organs, such as the heart, muscles, and brain. A deficiency in Mg can lead to conditions like heart disease, diabetes, bone disorders, and neurological impairment [6], [7]. At the same time, excessive levels of Mg in the human body can also be harmful [8]. While serum is commonly used to measure Mg in healthy individuals, it may not accurately reflect the actual Mg status due to strict regulatory mechanisms in the body, potentially leading to misleading results [9], [10], [11]. The majority of the body's Mg is stored in bones, muscles, soft tissues, and RBCs. RBCs, in particular, carry a comparatively high Mg concentration, with studies indicating lower Mg levels in RBCs among individuals following prolonged Mg-depleted diets [12], [13]. Additionally, Mg concentration in RBCs correlates with malignancy severity in cancer patients, although the underlying mechanism remains unclear [14], [15]. Thus, RBCs are the preferred specimen type for measuring Mg concentration in body stores [16].
Cu is a crucial micronutrient in the biological system, which may exist in the +1 or +2 valence state. It acts as a cofactor for oxidation–reduction reactions of different metalloprotein-dependent enzymatic reactions [17]. Cu can be obtained from shellfish, meat, chocolate, and whole grain [18]. Cu participates in approximately 300 enzymatic reactions in the human body by cycling between oxidized and reduced forms. It is predominantly absorbed in the gastrointestinal tract ileum, followed by transport to the portal blood, often binding with albumin, transcuprein, and/or metallothionein. It exhibits higher levels in women, particularly during pregnancy, oral contraceptive use, or estrogen treatment in menopause [19], [20]. Some essential biological functions of Cu include energy production [21], iron metabolism [22], neurotransmitter signaling in the central nervous system [23], catalyzation of melanin synthesis [24], prevention of oxidative damage [25] and promotion of angiogenesis [26]. Cu deficiency, resulting from malabsorption, Zn supplementation [27], or bariatric surgery, can lead to anemia, hematological abnormalities [28], cardiac damage [29], Menkes disease [30] and myeloneuropathy [31]. Excessive ionized, unbound Cu accumulation in the liver, kidneys, and brain can cause adverse effects through Cu-induced cellular toxicity [32]. Genetic disorders like Wilson disease and Cu-contaminated food or water can also induce toxicity [33] causing hepatic disease, skeletal abnormalities, neurodegenerative changes, and myocardial disease [34]. Laboratory measurements of Cu concentration in RBCs, serum and/or plasma and urine specimens are used to assess individuals at risk of toxicity and/or deficiency [35]. Cu is an essential element for erythropoiesis and competes with Zn for absorption, making RBC Cu concentrations reflective of intracellular levels, general homeostasis, and nutritional status.
Zn is an essential trace element that serves as a co-factor for more than 200 metalloenzymes, playing a vital role in biological pathways. It is distributed throughout the body's tissues, but is mostly found in muscle and bone [36]. Notably, Zn concentration in RBCs is 6–10 times higher than in plasma [37]. Deficiency in Zn, stemming from genetic diseases or poor dietary intake, can lead to various conditions, such as immune suppression, susceptibility to infections, hair loss, diarrhea, psychiatric or mental health impairments, and weight loss [38]. Conversely, elevated Zn levels due to supplementation can interfere with Cu absorption and result in excess concentrations of Zn, leading to conditions like acute respiratory distress syndrome, gastrointestinal distress, metal fume fever, anemia, and secondary copper deficiency [39]. Laboratory assessments for Zn deficiency or overdose use RBCs, serum, plasma, and urine specimens. The preference for RBC samples stems from their ability to reflect zinc's intracellular levels, providing insights into general homeostasis and nutritional status.
Accurately measuring Mg, Cu, and Zn within RBCs is crucial for assessing nutritional status and overall health. In the past, methods for measuring Cu and Zn in RBCs required outsourcing, leading to inefficiencies. Outdated technology hindered historical Mg measurements in RBCs. To address these challenges, this study introduces a newly validated inductively coupled plasma mass spectrometry (ICP-MS) method for simultaneous quantification of Mg, Cu, and Zn in RBCs, effectively overcoming past limitations. Laboratory methods play significant roles in assessing nutritional status and diagnosing metal toxicity, and ICP-MS is considered the gold standard for precise elemental determinations based on specific mass-to-charge ratios. The primary objective of this study was the development and validation of an ICP-MS method for quantifying Mg, Cu, and Zn in RBCs. Method development and validation experiments assessed accuracy, linearity, sensitivity, imprecision, and carryover. In addition, retrospective analysis was conducted on a dataset spanning one and a half years following assay validation, using post-validation patient data.
2. Materials and methods
2.4. Instrumentation
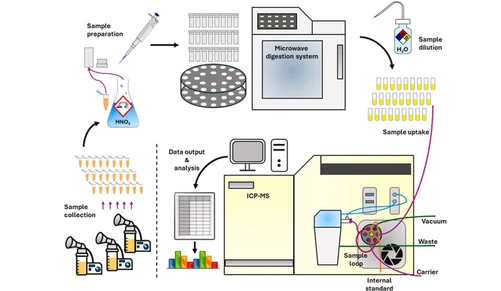
The multi-element RBC panel method employed an Agilent 7700 ICP-MS instrument coupled with a workstation and syringe injection CETAC MVX 7100 autosampler system. Helium gas was utilized to mitigate potential polyatomic interferences in this method.
2.7. ICP-MS analysis
The prepared 96-well plate containing the RBC samples was loaded into the CETAC MVX-7100 workstation autosampler, which facilitated the aspiration of diluted specimens into the ICP-MS system. The ICP-MS procedure involved introducing the aspirated samples into a plasma torch within an argon atmosphere, leading to aerosol ionization. The plasma torch, maintained at around 6000 degrees Kelvin with up to 2.5 kW of radio frequency power, enabled efficient ionization. To address potential interferences, helium gas was introduced at the collision cell entrance using the kinetic energy discrimination (KED) method. This helped eliminate polyatomic interferences that arise when combined atoms match the natural isotope's mass of the analyte. Other interferences, such as those from heavier elements with double charge states, were also evaluated (Table 2). These interferences could result in elevated element concentrations, necessitating correction during measurement. Targeted ions and interfering molecules underwent selective filtration through an energy filter to remove interfering ions from the desired analytes. These ions were then filtered by the main quadrupole, transduced into electrons, and amplified by the ion multiplier for quantification. The calibration curve used for quantifying the three elements was established by assessing ratios between varying amounts of calibrator components and a constant ISTD quantity.
3. Results
3.1. Accuracy and method comparison
Linear regression analysis was performed, with predefined criteria for slopes between 0.90 and 1.10 and intercepts below the LOQ for each element. Additionally, a correlation coefficient equal to or greater than 0.95 was mandated. All elements in the assay satisfied the specified accuracy criteria. Refer to Fig. 1 for the accuracy linear regression and bias plots of each element.
Journal of Mass Spectrometry and Advances in the Clinical Lab, Volume 34, 2024: Fig. 1. Accuracy study – Linear regression and Bias plots, magnesium (A), Copper (B) and Zinc (C).
3.6. Retrospective data analysis
In our retrospective patient data analysis, we examined information obtained through the new multi-element method. A total of 25,147 unique samples were collected for Mg, 1,823 for Cu, and 6,567 for Zn, covering various age groups from 0 to 105 years. The details of age and sex groupings are presented in Table 5(A), Table 5(B) for reference. Two-way ANOVAs were performed to evaluate the impact of age and sex on analyte concentrations. The results of the two-way ANOVAs indicated statistically significant effects of both age group and sex on the concentrations of Mg, Cu, and Zn (p = 0.003, p = 0.0003, p < 0.0001, respectively).
 Journal of Mass Spectrometry and Advances in the Clinical Lab, Volume 34, 2024: Table 5(A). Retrospective patient data analysis.
Journal of Mass Spectrometry and Advances in the Clinical Lab, Volume 34, 2024: Table 5(A). Retrospective patient data analysis.
Further analysis revealed that age group significantly influenced Cu and Zn concentrations (p < 0.0001), while sex had a significant effect on Mg and Zn concentrations (p < 0.0001). Additionally, Tukey’s HSD test was used for multiple comparisons, uncovering statistically significant mean concentration differences among nearly all pairwise groups of age and sex (p < 0.05), with a few exceptions. Specifically, differences in mean Cu concentration between adult males (≥18 to 105 years) and adult females (≥18 to 105 years), as well as mean Mg concentrations between adult males and young males (0 to < 18 years), were not statistically significant.
RIs were determined by age and sex based on standard normal deviation test results. Table 5(A), Table 5(B) present details including the total number of patients, age distribution, RI per element, and the percentage of the population within or outside of the adopted and calculated RI.
4. Discussion
Analysis of RBC specimens proves vital in assessing the nutritional status and potential toxicity of elements like Mg, Zn, and Cu. RBCs contain a variety of circulating elements, making them an ideal specimen type for evaluating element concentrations. Our laboratory employs this method to measure Mg, Zn, and Cu levels within RBC specimens. Prior to validating this multi-element method, measurements of Cu and Zn in RBCs were outsourced, and the reference ranges were adopted from the external reference laboratory. Furthermore, historical Mg measurements within RBCs were conducted using the PerkinElmer DRC ICP-MS instrument, which was eventually retired due to outdated technology, inadequate performance, and costly service contracts. This outdated instrumentation for Mg measurements presented limitations such as analytical inaccuracies, extended run times, and increased specimen volume requirements.
The new method was developed using an Agilent 7700 ICP-MS instrument coupled with a workstation and a syringe injection CETAC MVX 7100 autosampler system. Calibrators and quality control samples were employed to assess the acceptability of the calibration process, instrument drift, and test results. Our Reagent Lab prepares these QC and calibrators with varying levels of Mg, Zn, and Cu spiked into lysed red blood cells. This matrix-matched QC and these calibrators have significantly improved the analytical accuracy of this multi-element method.
We have presented data comparing combined and segmented age and sex groups, evaluating the currently adopted and calculated RIs for RBC Mg, Cu, and Zn. Our retrospective data analysis highlights the importance of incorporating age and gender-specific RIs for these elements in RBCs. It is essential to recognize the limitations of this retrospective analysis, including the lack of patient medical history, clinical conditions, inpatient/outpatient status, supplement intake, specific diagnoses, and reasons for laboratory evaluations. Furthermore, the dataset for Cu was relatively smaller than that for Mg and Zn, possibly reflecting lower test orders for Cu compared to the other elements. In summary, the ICP-MS method satisfactorily met the expected validation criteria for monitoring Mg, Cu, and Zn elements in RBC specimens.